

The cycle of creation, advent, and prohibition of New Psychoactive Substances (NPS) can be described as a series of actions and reactions by which each group participating acts correctly to maximize its end without considering the entire system. As a result, an unsatisfactory situation persists. A broad grasp of the problem allows suggesting solutions that maximize the greater good without heavy compromises to the active functions in the cycle.
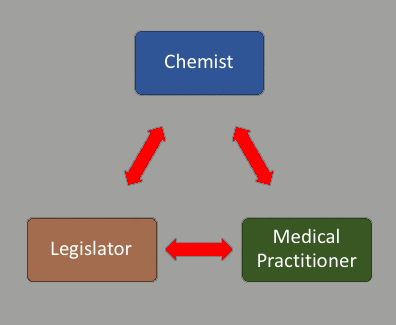
To describe the cycle, I will start with the invention of a new compound. This is done by chemists or people who employ them. This faction in the life cycle of an NPS (New Psychoactive Substance) is eager to maximize profits from the invention or discovery before it is banned. In their scramble to manufacture and distribute, they often neglect knowledge accumulation studies, which utilize methods such as in vitro bioassays, animal toxicology, and clinical trials, when preparing a pharmaceutical for market. Consequently, the new substance is used by a large, random population that knows nothing about it, and has no one to ask because the data normally generated was not created in haste to market. Moreover, the medical community is left uninformed as to how to provide treatment when the new compound is linked to a medical event.
The next stratum in the chain is the medical community. Its role in society is to maximize health. However, when faced with a medical problem linked to a substance about which nothing is known because no supporting literature was created, they feel, understandably, that the substance is impeding or hindering their work. As a result, they label it as potentially dangerous.
It is when the following function in the cycle – politicians learn about the potential threat embodied in this new substance - that they take action in the only way they know how: by legislating. Over and over again, politicians prohibit a substance only to complete the cycle and set the stage for its next iteration. I like to term this cycle ‘the NPS default recurrence’, and recognize that through no one’s direct fault or blame, it perpetuates a lot of misery and problems in our societies.
By breaking convention and acting differently, each faction of participants has the power to break the cycle and bring about a positive outcome on its own.
The chemists, by taking the time and effort to study the compound and its effect and by making this data available to the medical community, can stop the demonization of the compound and prolong its time on the market, possibly indefinitely.
The medical community, by tempering its panicked reaction, could quickly determine the appropriate treatment to provide for a medical event involving the new compound. Once the unknown becomes known, it is, to the medical practitioner, just another condition with its treatment. The handbook of the medical toxicology of drug abuse is complete with remedies to treat an extensive range of known drugs. These are applied often, and yet known drugs are not perceived as a potential threat. Their presence in society seems to be a necessary and tolerated fact (although undesired).
Finally, the politicians themselves could opt to impose a scheme other than prohibition, which would effectively allow the public to use the new compound from time to time but make it difficult enough so that consumption remained subdued, and did not go “out of control” or “get out of hand”. Examples for such schemes are the supervised injection sites operating in Switzerland, Portugal, Canada, and the Netherlands.
The NPS default recurrence is by far the most common outcome of the natural cycle of events. Examples such as Switzerland, Portugal, and the Netherlands (or New Zealand for that matter) are rare and unstable. They require an entire society, a massive group of people, to ignore their instincts and behave in a logical and controlled manner. And this, regarding a topic that is misunderstood, heated, and unsettling. That said, the few successes that have matured send a clear message that the effort is well worth making. A society in which many members choose more often than not to do what does not come naturally finds itself in a community that is forgiving of faults and mistakes, compassionate towards the weak, and striving thoughtfully toward the greater good.
The NPS default recurrence is difficult to break free of for many good reasons. The reactions that lead to it are automatic and do not require much thinking. The human brain often chooses the route of least cognitive effort over a more challenging one to achieve the greater good. Another factor is that the pressure and segregation inherent in modern life create the illusion of adversity between members of society who play different roles. This adversity drives a propensity towards uncompromising views and away from the tolerance and understanding required to break the recurrence.

On the other hand, the recurrence can be broken by anyone caught in the cycle.
It is when the chemist chooses to delay gratification over “quick and dirty” results and to collect data first that the recurrence is broken.
It is when the medical professional chooses to react by studying the problem and seeking a solution, rather than ignoring it out of fear of the unknown, that the recurrence will be broken.
It is when politicians choose the more difficult path of creating the least harm over unyielding prohibition that the recurrence is broken.
Breaking the recurrence requires a clear personal sacrifice in exchange for a blurred contribution to the greater good. That is why it is the exception and not the norm. However, if we understand the cycle, explain it clearly, diligently, and patiently, and spread the word, we may be able to influence those whose decision it is to break the recurrence.
This is both an analysis and a call to action, intended to work in tandem to bring clarity to decisions that have been made too often in error.